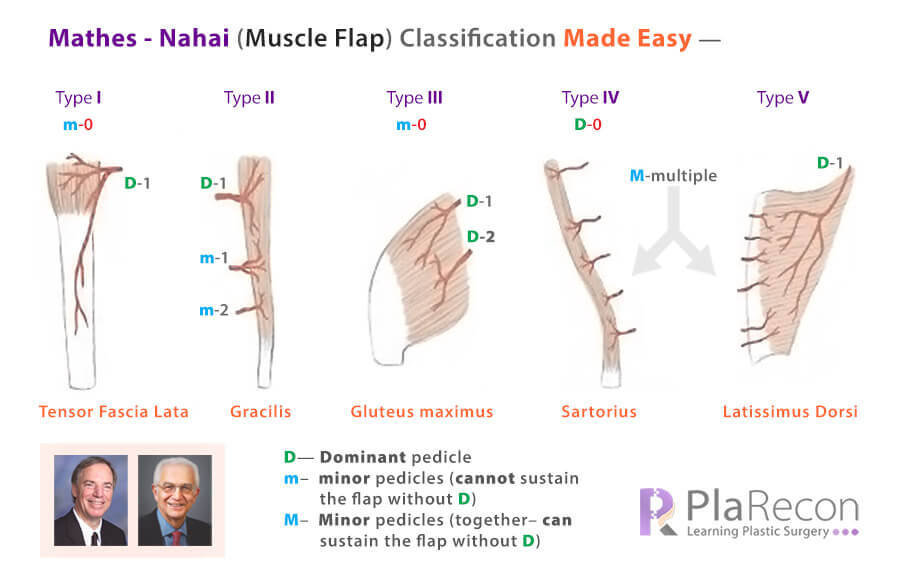
The vascular anatomy of muscles was classified into 5 types by Stephen J. Mathes and Foad Nahai in 1981. It is still the most accepted classification used for choosing and designing a muscle and musculocutaneous flap for its use in reconstructive surgery. The clinical applications of Mathes – Nahai classification are listed at the end.
The classification and examples of each type are quite difficult to remember and volatile for novices but questions based on this classification are most frequently asked in exams- especially MCQ-based ones.
The Muscle flaps have been divided into 5 types based on these 5 variables:
- regional source of the arterial pedicles,
- their size,
- their number,
- their location in relation to the origin and insertion of the muscle,
- angiographic patterns of the internal muscle vessels.
To aid memory (& esp. to get the MCQs correct), have shared below the mnemonics, patterns, picmonics, colors etc. (disclaimer: some are really silly but effective!), that have helped us get them right most of the time. Surely, each one of us would have figured out some way or the other to remember this long list – Please share your’s in the ‘comments section’ below the best one’s will be updated in this post with your name by the side.
⭐ Salient Points:
- A Dominant pedicle can sustain the entire flap while a Minor pedicle can sustain only a portion/segment of the flap.
- The difference between Class II and Class V is that in Class II– the minor pedicles together are not enough to sustain the whole muscle flap in case the Dominant pedicle is sacrificed, while in Class V– the Minor pedicles together can (like in Class IV).
- Hence, in Class V, the Minor pedicles are also called ‘secondary’ supply. They generally:
- have a source of circulation different from the dominant pedicle,
- enter the muscle from an end opposite to the site of entry of dominant pedicle.
| Mathes-Nahai Type | Dominant pedicle(s) | Minor pedicle(s) |
|---|---|---|
| I | 1 | 0 |
| II | 1 | 1 (or more) |
| III | 2 | 0 |
| IV | 0 | Multiple |
| V | 1 | Multiple |
💡 The Table above simplifies the types I-V where you can see an incremental rise in number patterns » 1-0 ⟶ 1-1 ⟶ 2-0 ⟶ 0-multiple ⟶ 1-multiple [Mnemonic]
So, that solves one part. Now, we will try and remember the loads of examples under each type.
NOTE: Few authors include parts of the intestine, omentum and fibula (not muscles) in the classification, possibly since they have a similar vascular pattern and behaviour. But in our description below, we will include them separately(+) at the end of each type.
Type I- Single Vascular Pedicle
- Tongue: Medial and lateral Genioglossus, Hyoglossus, Longitudinalis linguae, Styloglossus, Transversus and verticalis linguae
- Hand: Abductor digiti minimi, Abductor pollicis brevis, First dorsal interosseous; [💡Foot muscles → II]
- Arm: Anconeus; [Triceps → II]
- Hip: Deep circumflex iliac artery (DCIA)
- Thigh (Lateral): Vastus lateralis, Tensor fascia lata [💡 Antero-medial, Posterior muscles → II; EXCEPT Sartorius→ IV]
- Leg: Gastrocnemius; [💡Soleus → II]
+ G.I. (Intestine): Jejunum, Colon [Not muscles. Note: Omentum → III]
💡Mnemonic: Tongue Lying-Tied (Lateral-Thigh) Deep (DCIA) In (Intestine) Hand.

Type II- Dominant Vascular Pedicle and Minor Vascular Pedicle(s)
- Neck & Back: Platysma, Sternocleidomastoid, Trapezius
- Arm, Forearm: Brachioradialis, Coracobrachialis, Triceps, Flexor carpi ulnaris, Flexor digitorum brevis
- Thigh (Antero-medial, Posterior): Rectus femoris, Vastus medialis, Gracilis, Hamstring (biceps femoris)
- Leg: Soleus + Lateral compartment (Peroneus brevis, Peroneus longus)
- Foot: Abductor digiti minimi, Abductor hallucis
💡Mnemonic: Class II is linked to→ Class I [Except for Neck & Back]
Type III- Two Dominant Pedicles
- Head: Temporalis, Orbicularis oris
- Thorax: Intercostal, Pectoralis minor, Serratus anterior
- Abdomen: Rectus abdominis
- Buttock: Gluteus maximus
+ G.I.: Omentum [not muscle]
💡Mnemonic (Indian)- for Abdominal muscles: III IV V→ Aishwarya REI [Rectus abd, Ext Oblique, Int oblique]
[REI is spelt wrongly on purpose. To aid memory, here’s a snapshot of a famous Bollywood scene]
💡Mnemonic (for Glute max in Type III): Three Glutes!
[The illustration is anatomically wrong on purpose 😃]
Type IV- Segmental Vascular Pedicles
- Abdomen: External oblique
- Thigh: Sartorius
- Leg: Extensor digitorum longus, Extensor hallucis longus, Flexor digitorum longus, Flexor hallucis longus, Tibialis anterior
Type V- Dominant Vascular Pedicle and Secondary Segmental Vascular Pedicles
- Thorax: Pectoralis major, Latissimus dorsi [Rest of the Thorax muscles → III]
- Abdomen: Internal oblique
+ Leg: Fibula [not muscle]
💡Aid to Memory: Flaps for Oncoplastic reconstruction: Pec major, Fibula for H&N and LD for Breast.
💡Some Salient PATTERNS to help remember:
- Muscles of the Head region (in III) come after that of the Neck (in II).
- Muscles of the Thorax are in III and V.
- No Muscles of the Limbs in III.
- Upper limb→ muscles of the arm are present in I and II, of the forearm in II, and of the hand in I.
- Lower limb→ muscles of the thigh are present in I, II and IV, of the leg in all except III, and of the foot in II.
Clinical applications of Mathes – Nahai classification
- It helps predict the arc of rotation of pedicled muscle flaps.
- Muscles classified as types I, II, III, and V can survive solely on their dominant pedicle and hence are more amenable to rotation or transposition than a type IV flap. In addition,
- Type III (no comments on type V) muscles have two potential arcs of rotation based on their two dominant pedicles.
- It also aids in the prediction of viable skin territories. Types II, III, and IV muscles are at risk of skin necrosis if distal segmental or minor pedicles are divided, whereas skin survival in type V flaps is robust.
If you liked the post and the (silly) mnemonics, do subscribe for more. Please share below your mnemonics for this classification too in the comments section. You may also like to see Classifications for Fasciocutaneous flaps made easy!
References (for further reading):
- Mathes SJ, Nahai F. Classification of the vascular anatomy of muscles: experimental and clinical correlation. Plast Reconstr Surg. 1981;67(2):177–187.

Tutorials & tips in Plastic Surgery
+ Weekly updates of high-quality webinars!

{kind=link}